NTES FROM NB 2023
http://www.macmillan.org.uk Booklets detailing all available trreatments
http://cancerhelp.cancerresearchuk.org Includes current trials in progress
http://www.cruk.org is Cancer Research UK
http://cancerhelp.cancerresearchuk.org/type/melanoma/treatment
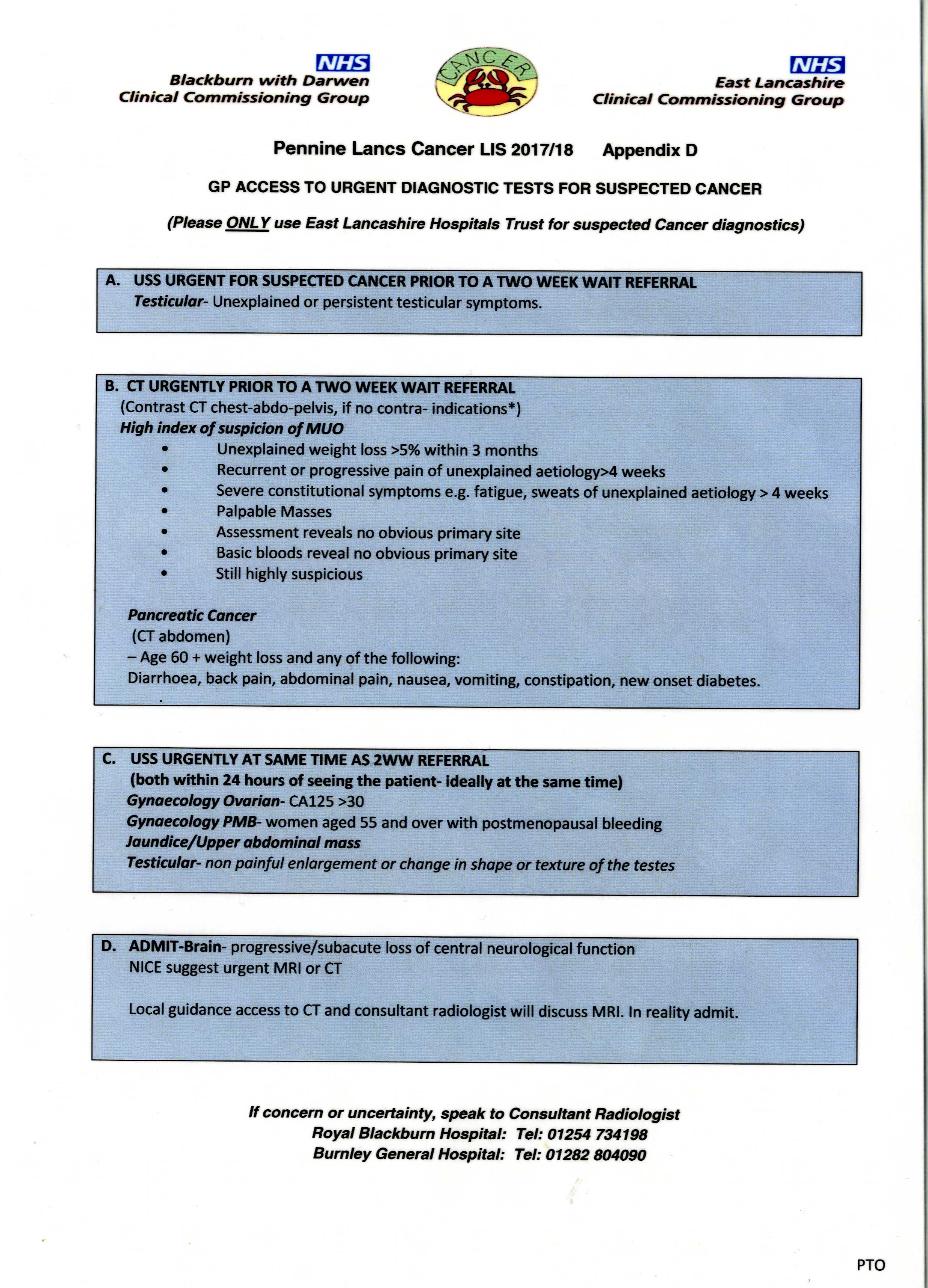
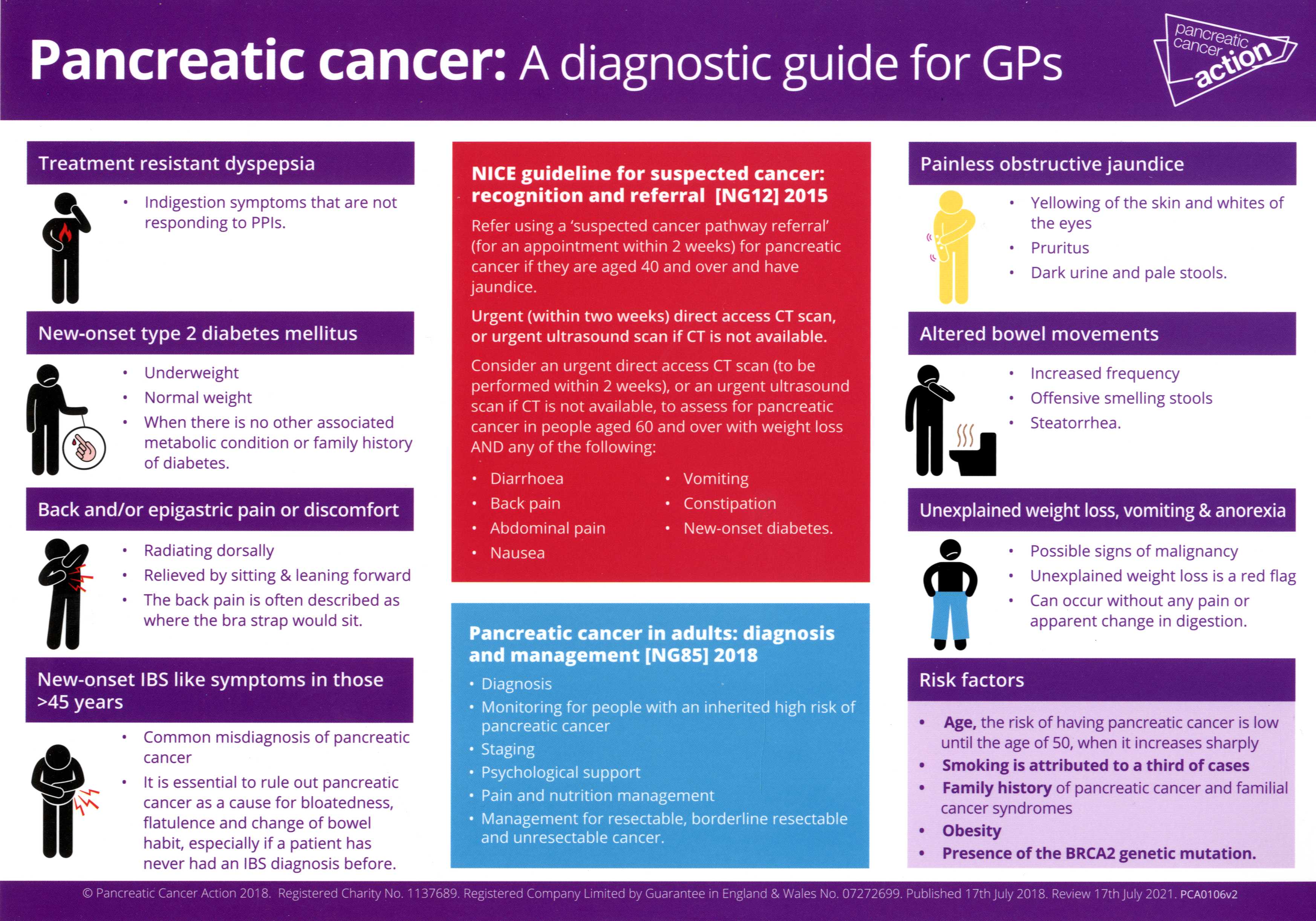
http://www.nice.org.uk/guidance/NG12/chapter/1-recommendations
http://www.nice.org.uk/guidance/index.jsp?action=byTopic&o=7165 Lists Cancers Includes All Sorts of Treatments Current
http://cancerlancashire.org.uk/GP-zone/gp-resources.php
NAEDI FAST TRACK REFERRAL FOR CANCER
Patient.co.uk also has up to date information on each cancer
KNOW FOR SURE LEAFLET ABOUT SYMPTOMS TO WATCH FOR http://www.nhs.uk/cancer-symptoms/Pages/generic-cancer-signs.aspx
www.cancerlancashire.org.uk has various guides on services e.g.EastLancsCancerInfoGuide2011
LUNG CANCER MASTERCLASS 17 Sept 2013
American Cancer Society http://www.cancer.org
NCCN GUIDELINES FOR PATIENTS http://www.nccn.org/patients/guidelines/cancers.aspx
CANCER DECISION SUPPORT PROGRAMME http://www.macmillan.org.uk/Aboutus/Healthandsocialcareprofessionals/Macmillansprogrammesandservices/Earlydiagnosisprogramme.aspx

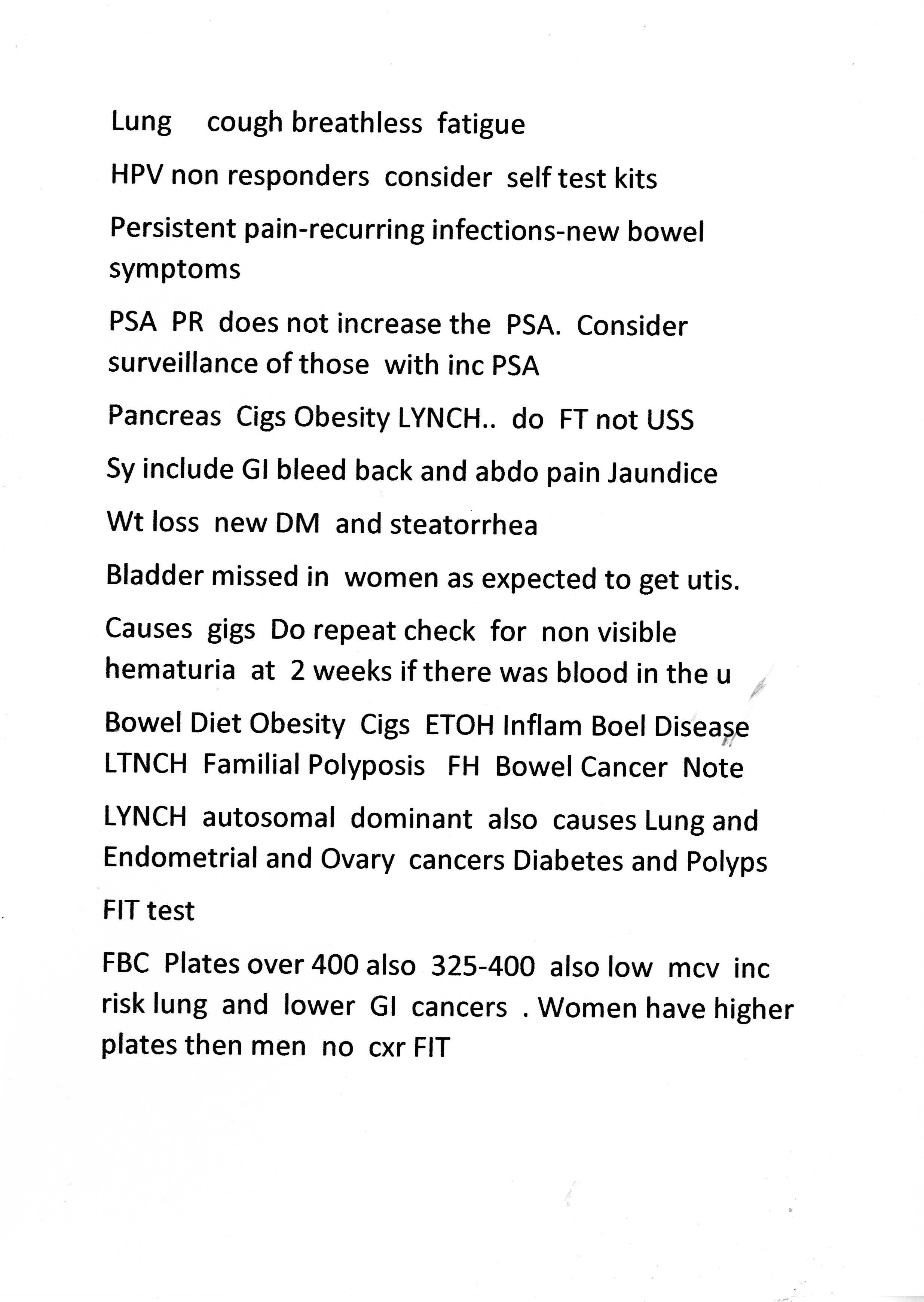
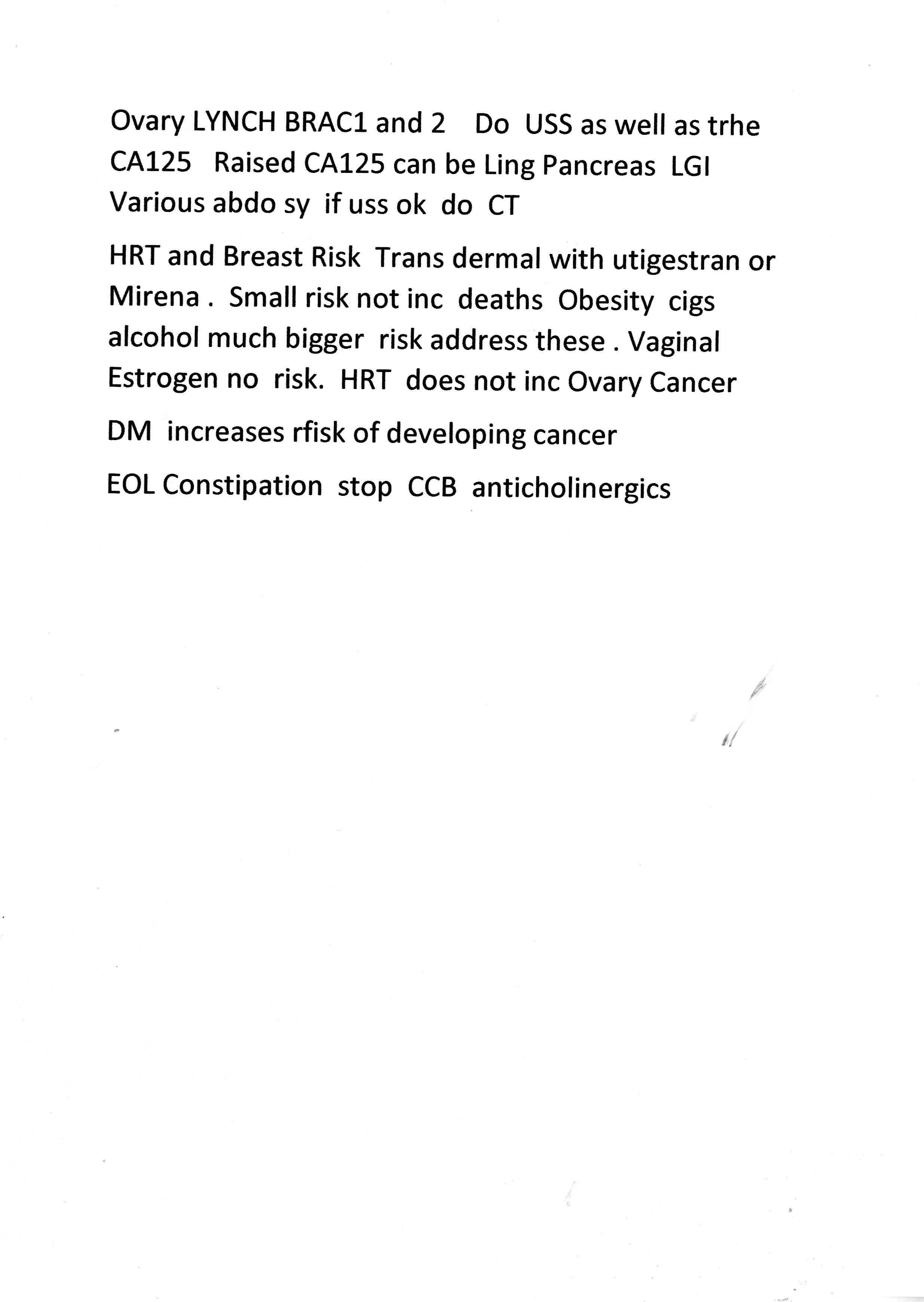
MORE CANCER REFERRAL SUGGESTIONS FRON CCG JUNE 2015
Lung
·
Clinically pneumonia do repeat CXR at 6 rather than immediate 2ww referral
·
Suspected TB send
to TB clinic not 2ww.
·
Pleural
effusion usually unilateral which is more likely to be sinister as compared to
bilateral effusion with history of CCF- add clinical details and patient can go
straight to pleural list.
·
If patient has
got high suspicion of having lung cancer and even if CxR is reported as normal
please still refer the patient to 2 week rule clinic.
Urology
·
Haematuria- always check for infection. MSSU positive treat the infection
·
Referral with an
elevated PSA checked during a UTI or symptoms suggestive of a UTI as this will
often give an abnormal result. The only exception would be if the Prostate feels
obviously malignant but both of these factors need to be specified in the
referral.
Check the urine, treat any
infection or suspicion of infection appropriately and leave for at least one
month after treatment before testing the PSA.
·
Referral
with a single, slightly elevated age specific PSA test with a normal feeling
Prostate. The level of PSA can fluctuate and if a second test is normal and the
Prostate feels normal then urgent investigation is probably not required.
In this situation, repeat the PSA test in 1-3
months and only refer if the level remains elevated or is rising.
·
Consider value in
referral with a slightly elevated PSA level in men over 75 years of age or with
significant co-morbidities meaning their overall life expectancy is probably
less than 10 years. The exception is where patients have symptoms suggestive of
locally advanced or metastatic disease and have a frankly malignant feeling
gland.
Lower GI
·
Rectal bleeding
with anal symptoms or patient less than 40 without family history --straight to
flexible sigmoidoscopy
·
Decreased
defaecation and harder stools Routine referral if usual treatments for
constipation fail
·
Abdominal pain
without evidence of obstruction or mass-
routine referral
Hepatic/pancreatic/biliary
·
Not to
refer none malignant problems as 2ww (e.g. incidental findings found on a scan).
Can use options other than 2ww: routine referral; urgent referral or telephone
advice.
Head and
Neck
·
Small round
simple mouth ulcers in young non-smoking patients are very common and very
unlikely to be cancer; routine management/check for anaemia
· Recognize common benign neck lumps e.g. sebaceous cysts.
MACMILLAN CANCER FILES
http://www.guidelines.co.uk/malignant_disease_macmillian_cancer_referral_toolkit#.Vkug9xKdFlw
http://www.nice.org.uk/guidance/ng12
http://www.elmmb.nhs.uk/search/?q=syringe+driver




Referral Forms www.eastlancshospice.org.uk
www.cqc.org.uk End of Life Care
Anticipatory Rx
Pain
Nausea
Agitation
Dyspnoea
Respiratory Secretions
ELMMB Guidance on Syringe Drivers and Symptom Control
Morphine Midazolam Cyclizine Hyoscione Hydrobromide
Do not use saline with Cyclizine
Do not mix Cyclizine with Oxycodone
Max capacity of syringe driver is 22 ml
OPIATES IN SG DRIVER
Halve the oral dose
Oxycodone = twice potency of Morphine
Fentanyl 75mg= 180 mg oral or 90 mg S/C Morphine also takes up to 3 days to come on or go off so don’t stop just add morphine as S/C
PRN S/C Morphine = 1/6 of the 24 hour dose
NICE CANCER GUIDELINES 2015 http://www.cancerresearchuk.org/health-professional/learning-and-development-tools/nice-cancer-referral-guidelines